Movement Disorder Surgery: Neurophysiology

Stereotactic or “functional” neurosurgery for Parkinson's disease (PD), dystonia, tremors, and other movement disorders has re-emerged as a standard form of treatment over the last decade due largely to improvements in surgery, brain imaging, and advances in our understanding of brain physiology. Abnormalities in the circuits that connect different subcortical nuclei of the brain, specifically the internal globus pallidus (GPi), part of the ventral thalamus (Vim), and subthalamus (STN), are believed to play major roles in the development of movement disorders.

Stimulating these dysfunctional circuits with implanted deep brain stimulators (DBS) has proved therapeutic for many patients. Although there are some indirect excitatory effects, paradoxically, DBS works primarily by inhibiting neural firing patterns that are overactive and disordered in the GPi, Vim, and STN. That is, the stimulator acts by “numbing” the source of the problem and altering its signal to the rest of the brain.
The Clinical Motor Physiology Laboratory has been involved in movement disorder surgery since 1995. Our team is responsible for the intra-operative guidance of DBS placement using neurophysiological methods as well as the quantitative pre- and post-operative physiologic assessments.

As part of the Movement Disorder Surgery Center, our colleagues include Dr. Blair Ford and Dr. Guy McKhann. Linda Winfield is our DBS programming nurse who ensures that the patients’ stimulators are optimally adjusted. We have worked particularly closely with Dr. Lucien Côté who was a major influence in the development of our intra-operative physiological guidance system. The pre-op and post-op testing, as well as the intra-operative mapping and monitoring team.
Today, DBS surgery is considered for patients with moderate to advanced PD or related disorders, who retain medication responsiveness, but have an overall worsening course or suffer from serious side effects. Similarly, patients with intractable essential tremors or severe dystonia, particularly those carrying the DYT1 gene, also benefit from DBS therapy. The list of potential neurological indications for DBS is growing rapidly.
Targets for DBS placement are quite small (only millimeters across), located deep inside the brain, and not always easily identifiable by MRI or CT imaging. To address these issues, we combine mapping and monitoring techniques in the operating room and compare the clinical results with our pre-operative evaluations to assist in the accurate identification of DBS implantation targets.
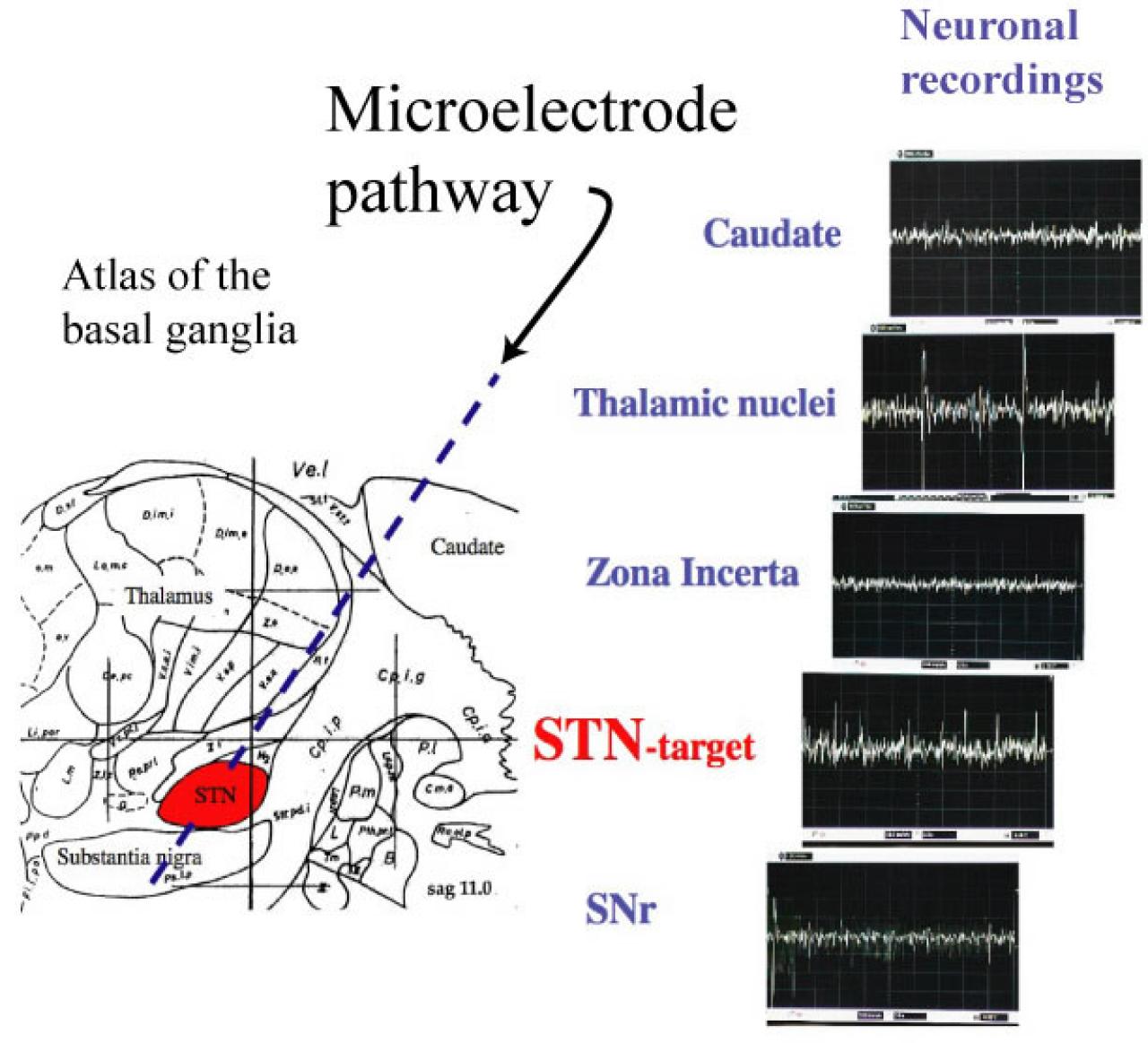
Mapping uses microelectrode probes to provide highly precise, sub-millimeter localization of the desired DBS targets. This is accomplished using the real-time recordings in the operating room of the electrophysiologic “signatures” of neurons and neighboring white matter tracts. All regions of the brain from more superficial areas to deep sub-cortical nuclei including the GPi, Vim, or STN exhibit recognizable waveforms, firing patterns, and changes in relation to clinical manipulation or specific stimulation.
Patients are also monitored via continuous collection of additional physiologic data, such as EMG to measure muscle activation patterns from tremors or other involuntary movements, or visual evoked responses to determine the relative location of the optic tract, a critical anatomic landmark in GPi surgery. Monitoring in this manner provides adjunctive information on the status of the mapping procedure and final DBS implantation. Procedures are typically performed with the patient awake but mildly sedated so that the effects of voluntary motion and responses to various sensory inputs are possible.
In their aggregate, these physiologic methods help determine the exact dimensions, shape, and depth of the DBS targets, as well as their relationship to neighboring neurons and white matter tracts. This allows for optimal DBS placement and contributes to the accuracy, safety, and overall outcome efficacy of DBS surgery.